
Implant considerations based on physical and anatomical features

Thanks to all the progress made in implantology, dental implants are becoming more and more similar to natural teeth. However, it must be taken into account that there are a series of differences that limit the behaviour of an implant, since it is a prosthetic element inserted in a living organism.
Among all the differences, the following should be highlighted:
- Material composition. The natural tooth is a living tissue while the implant is made of titanium.
- The way in which it is attached to the bone. The natural tooth is held in place by the periodontal ligament, whereas the implant is attached directly to the bone thanks to osseointegration: a mechanical union through which the bone cells adhere to the surface of the implant, thereby progressively consolidating its attachment to the maxillary or mandibular bone.
As a result, the natural tooth reduces the forces that appear around the bone ridge. The dental implant, on the other hand, does not.
Compositional materials of dental implants
We can classify implants according to the material they are made of.
Titanium Dental Implants.
Titanium is the material most traditionally used for dental implants as it is a metal of great hardness and highly biocompatible that bonds with the bone through osseointegration. For this reason, along with its excellent resistance to corrosion, DESS® Implants are made of Titanium Grade 4.

It is important to highlight that once the titanium comes into contact with the air, a superficial layer of titanium oxide begins to form, which is precisely the biocompatible element that ensures that the implant becomes a bioactive part of the physiological environment. This surface layer grows considerably in the mechanization process of dental implants, a process in which titanium reaches high temperatures that favor oxidation.
Titanium meets the most important qualities relevant to Biomedicine:
- Corrosion resistance
- Biocompatibility
- Bioadhesion
- Elasticity coefficient as close to the bone as possible.
- Material resistance
Zirconium Dental Implants
The technique used for zirconium implants is biointegration. In this process, instead of a mechanical bonding, as in the case of osseointegration of titanium implants, we are dealing with a chemical bonding that occurs through a layer formed between the surface of the bone and the surface of the implant.

In addition to the material and the bone union method, there are other characteristics of the implants that are equally relevant, such as the thread design, the implant collar and connection, the dimensions and shape of the implant, or the treatments applied to the surface (sandblasting + acid etching).
Osseointegration
The concept of osseointegration was first introduced by Dr. Branemark in the 1950s. It refers to the process where a surgical implant, such as a dental implant, directly and securely attaches to living bone without any intervening layer of soft tissue. This connection is both functional, meaning the implant serves its intended purpose effectively, and structural, indicating it integrates with the bone structure. Because the bone and the implant bond tightly together, there is no movement between them, ensuring the implant is stable and immobile.
Therefore, the success rate in a dental implant process is directly related to the osseointegration process and the way in which this surgical technique is developed.


Endosseous implants are the most commonly used type of implant in dental implantology since, once osseointegrated, they allow moving on to the loading and prosthetic restoration phase. This is why DESS® Implants: ACTIVE HEX and CONICAL BLT are endosseous implants.
Implant body morphology classification
Implant stability is a parameter directly related to its quality, since the study between the geometric relation and the mechanical properties of implants is what provides a rigid attachment of the implant to the bone tissue and therefore, an improvement in the stability, durability and performance of the implant.
In addition, the implant design determines the area where the forces that the implant mechanism withstands during its lifetime are distributed, which is one of the pillars for achieving high success rates in implant dentistry. The implant body is generally composed of an external thread that simulates the mechanism of a screw to achieve attachment between elements. However, according to the geometry of the body design, they can be classified mainly into: conical/tapered implants and cylindrical or straight-walled implants.
Tapered implant: this is the name given to implants that simulate the natural shape of the tooth root. The development of this morphology of the implant body is one of the most important developments in implant dentistry.
DESS® Implants are conical in shape.


Cylindrical implant: it is a type of implant characterized by parallel sides.

Implant connections
The technological evolution in implant design has led to various ways of achieving the structural connection between the abutment and the implant body. There are three types of connections to be highlighted in modern implantology.
External connection
External connection implants were among the first to be developed by Dr. Branemark during his research on osseointegration. This type of connection is characterized for connecting the abutment and the body of the implant externally using a screw. The geometry used varies according to the manufacturer (hexagonal, octagonal, circular, etc.).
The problem with this type of implant is that sometimes the screw loosens due to occlusal forces (chewing, dental clenching, etc.) and can even deform or break.

Internal connection
Internal connection implants arose in response to the need for evolution of the external connection type.
This type of connection is characterized by an internal connection between the abutment and the body of the implant and just like the external connection implants, the geometry of these varies widely (hexagonal, triangular, cone, etc.).
This type of connection covers the disadvantages offered by the external connection, providing greater stability and esthetics to the implant.
DESS® Implants, ACTIVE HEX and CONICAL BLT both have an internal connection.
Internal connection dental implants have been manufactured for about twenty years and include a kind of pivots that penetrate inside the implant, thus increasing the resistance to occlusal forces. Consequently, the chances of screw loosening are reduced, making it practically impossible for the connection screw to break or deform.

Morse cone connection
With this structure a union between implant and abutment is achieved through the friction offered by the walls of both parts, due to their conical shape.
This term is known as cold welding, forming a blockage between both parts and increasing the resistance of the structure, achieving a reduction of the loosening of the implant-abutment connection. One of the limitations of this connection is that it is not indicated for use in bone thicknesses below 7mm.
As a consequence of all the technological advancement in recent years, biomechanics is considered one of the most active disciplines in the field of research and development, which is gradually expanding its scope of application.

Bone densities
The bone is a hard and resistant structure made up of different tissues. According to biomechanics, bone is composed of cortical bone and trabecular bone.
A distinction can be made between cortical bone, made up of a more compact and resistant tissue that has a higher density, and trabecular bone, which has a more prorouse tissue with lower density and which regenerates at a higher speed.
The structure where the implant is installed and supports it is what is known as the external architecture of the bone, while it is the internal architecture that determines the resistance and quality of the bone. These two parameters, which are directly related, constitute the essence of success and are crucial at the time of making decisions such as implant design, surgical procedure and healing time/osseointegration.
Based on the classification made by Dr. Carl. E. Misch the four bone densities are:
Type I Density (Very hard bone)
This is the most resistant density of all, since it hardly shows any porosity in its structure, so most of the bone composition is of the cortical type.


Type II Density (Hard bone)
In the second density type there is already a somewhat porous structure that presents the trabecular bone. The pore orifices in Type II are quite small in size compared to the other densities. However, the cortical structure forms the largest percentage in its composition so the level of strength and stability is quite high.

Type III Density (Soft Bone)
It is formed by a thin layer of cortical bone and a thicker layer of trabecular bone. As a result, this type of density presents a proportion of porosity in its structure.


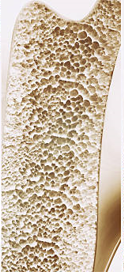
Type IV Density (very soft bone)
Density four is what would be equivalent to a mostly porous structure with a very thin layer of cortical bone.


Conclusion
Within the existing implant typologies on the market, DESS, always looking for the best quality options, launched its two implant systems: ACTIVE HEX and CONICAL BLT.
DESS® Implants features:
- Manufactured in Titanium Grade IV
- DESS® quality and technology
- Internal connection
- Conical implant body morphology
- Pure switch concept: 100% Compatibility. ACTIVE HEX is 100% compatible with NobelActive ® Implant System & components and CONICAL BLT is 100% compatible with Straumann ® BL Implant System & components.
- High Primary Stability
- Zero Waste implant: Packaging made of recycled and recyclable material.